Cycle 2 Recap

Cycle 2 Recap: The Data Is Starting to Have a Shape
Cycle 2 ran April 29 through May 26, 2026 and included three serum draws, twenty-one Inito readings, and one very tired luteal phase.
The short version: the protocol is producing an estradiol curve that broadly follows the shape of a natal menstrual cycle, serum data is starting to confirm what the urinary monitoring has been suggesting, and progesterone made its presence extremely known.
The E2 Curve
This is the cycle where the Inito coverage finally got dense enough to see the full shape. Twenty-one of twenty-eight days have readings, compared to ten out of twenty-three eligible days in Cycle 1. That's a meaningful jump, and it changes what you can actually read from the data.
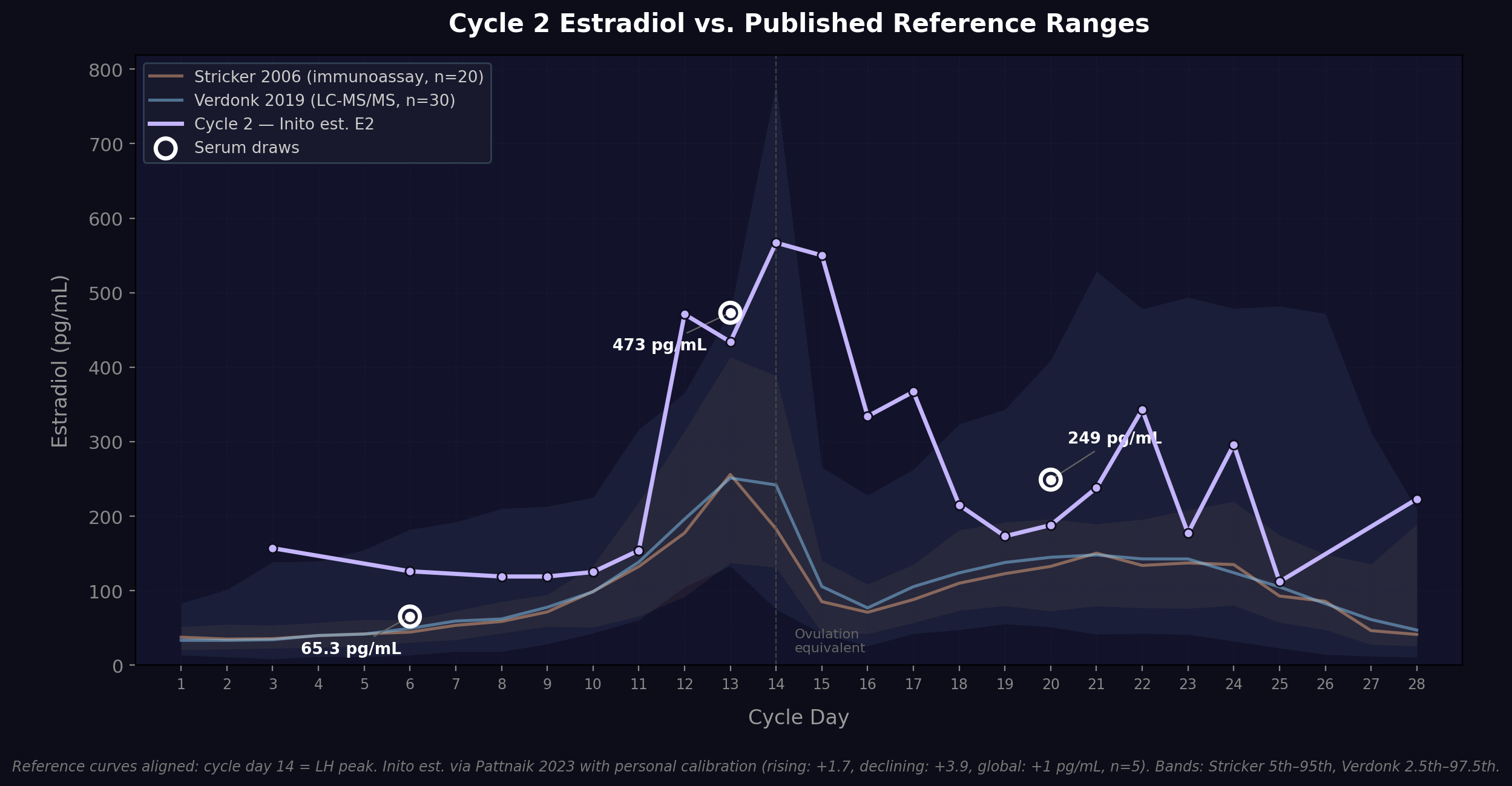
The trajectory: follicular baseline sits around 84-120 ng/mL E3G through the first week, then the 4mg injection on CD10 drives a steep climb. How steep? CD11 to CD12 goes from 119 to 409 ng/mL. A 3.4x increase in a single day. Peak lands at 498 ng/mL E3G on CD14, which is day 4 post-injection. After the peak, E3G drops through the early luteal phase, then a secondary rise builds from the third and fourth injections before declining through the end of the cycle.
That sequence (low baseline → mid-cycle peak → dip → secondary luteal elevation → decline into withdrawal) is the natal menstrual E2 pattern. The mechanisms are different: the peak is driven by injection pharmacokinetics rather than a dominant follicle, and the luteal rise comes from stacked injections rather than corpus luteum output. But the levels land in the right ranges, and the shape is recognizably cyclical.
The one structural difference worth noting is the follicular nadir. A natal cycle starts with E2 down around 20-50 pg/mL. Mine sits at 65 pg/mL on CD6 (serum-confirmed). That's residual carry-over from the prior cycle's last injection. The protocol doesn't produce a true washout, and whether that matters functionally (receptor resensitization, tissue remodeling cues from the low-E2 window) is an open question.
Serum Validation
Three draws this cycle, the most in a single cycle so far.
CD6 (before first injection, 2mg): E2 at 65.3 pg/mL. This reproduces the Cycle 1 trough. Having a consistent early-follicular baseline across two cycles is useful; it means the starting point is stable and not drifting.
CD13 (day 3 post second injection, 4mg): E2 at 473 pg/mL. That's approximately the 85th percentile of the Verdonk LC-MS/MS reference range for the ovulatory phase. On the same day, Inito reads 375 ng/mL E3G, which underestimates the serum value. This is the direction-dependent lag showing up again: when serum E2 is rising rapidly, urinary E3G hasn't caught up yet.
CD20 (day 5 post third injection, 3mg): E2 at 249 pg/mL, squarely within the natal luteal reference range. This is the first mid-luteal serum datapoint in the study, and it came from Labcorp via LC-MS/MS rather than CPL's immunoassay. That creates a cross-lab, cross-methodology comparison within the same cycle, which is both scientifically interesting and a genuine limitation when comparing values directly.
The CD20 draw also gave me progesterone at 4.34 ng/mL (lab reported as 434 ng/dL; converted for unit consistency). This was drawn the same morning after a 400mg vaginal dose, so it's a post-dose absorption datapoint rather than a steady-state level. But it confirms that vaginal micronized progesterone is absorbing through peritoneal neovaginal tissue and reaching measurable serum concentrations. That's essentially undocumented in the literature.
FSH across the three draws: 4.1 → 2.7 → 0.53 IU/L. LH on CD20: 0.47 mIU/mL. Gonadotropin suppression deepens progressively as cumulative estrogen exposure builds through the cycle.
Progesterone Hit Different
The single most noticeable subjective change in Cycle 2 was the fatigue. I was not prepared for how hard the luteal phase would hit.
The P4 protocol starts at 200mg nightly on CD15, then escalates to 400mg twice daily on CD19. My Clue logs from CD19 through CD23 are a wall of "exhausted." Five of the seven days I tracked during the 400mg BID window got that label. The timing is clean: fatigue onset maps almost exactly to the dose escalation.
The mechanism isn't mysterious. Micronized progesterone metabolizes to allopregnanolone, which is a GABA-A receptor agonist. It's functionally a sedative. This is one of the most reliably reported side effects of progesterone supplementation, and now I have my own n=1 confirmation.
Breast tenderness tracked alongside the fatigue from CD17 through CD21. Also classic progesterone.
The PdG data from Inito shows a readable dose-response curve: follicular baseline around 0.1-1.0 µg/mL, early luteal on 200mg nightly around 2.0-2.5, then after escalation to 400mg BID it climbs through 3.4, 4.4, and peaks at 4.84 on CD23. You can see the protocol in the metabolite data.
Wearables
Skin temperature might be showing a progesterone-mediated thermogenic signal. The luteal window (CD18-CD23) runs 36.41-36.62°C, with the cycle peak at 36.62 on CD20. Follicular readings cluster lower (35.45-36.26). Missing data on several follicular days makes it harder to call definitively, but the pattern is suggestive and the mechanism (progesterone → hypothalamic thermoregulatory setpoint shift) is well-established.
Resting heart rate shows slight luteal elevation (73-75 bpm on CD18-CD20 and CD24 vs. mid-60s in the follicular phase), but the signal is noisy. HRV is all over the place (10-59 ms) with no obvious cyclical pattern.
Adherence
Estradiol cream is still the problem child. Five of eight scheduled applications missed on their scheduled day. The pattern isn't random: it's a twice-weekly topical that doesn't have the same "event" quality as an injection or a nightly vaginal insert. It's easy to forget, and once you've missed the window, there's no natural prompt to catch it.
More broadly, adherence has a shape across the cycle. The first five days and the last five days are where things break down. The ovulatory and early luteal core (CD8-CD21) is where the protocol runs tightest. This probably reflects the subjective reality of the cycle: the middle of the cycle is when things feel most routine, and the transitions at both ends are where structure loosens.
P4 adherence in the late luteal phase created a gradual taper instead of the designed sharp cutoff. Missed PM doses on CD23 and CD25, then both doses missed on CD26 (one day before the designed withdrawal window). The protocol calls for a clean stop at CD27; what actually happened was more of a stepped drawdown over the last four days.
VagiBiom adherence also degraded late: four consecutive missed days to close the cycle (CD25-CD28). The loading protocol works better when there's energy and routine to support it.
Mood
Two clusters show up in the Clue data. Early follicular (CD3-5) logged sad, angry, irritable, anxious, and sensitive. The luteal phase (CD17-22) logged a similar set: irritable, anxious, sensitive, sad. Withdrawal day (CD26) added insecure to the mix.
The eleven-day gap in self-reporting from CD8-CD18 means the ovulatory window is a blind spot for mood data. This is one of the coverage gaps I want to close in future cycles.
Cycle 1 vs. Cycle 2
A few direct comparisons worth noting:
The early-follicular E2 trough is reproducible across both cycles. That's a stable baseline. Inito coverage improved dramatically (21 days vs. 10). Cycle 2 produced the first luteal-phase serum data and the first cross-methodology lab comparison. The full E3G curve shape is visible for the first time.
And the fatigue is new. This wasn't something I noted prominently in Cycle 1, and it was the dominant subjective experience of the Cycle 2 luteal phase.